
( This is an updated version dated 17th April’2016 with answer to some questions from esteemed readers. )
What is the controversy around A1 and A2 β -casein in milk?
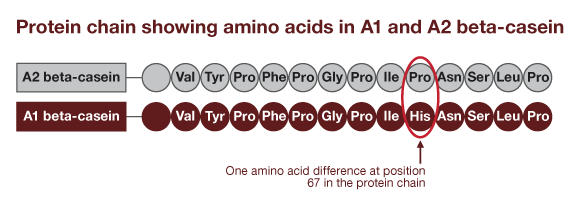
β- Casein is one of the major proteins in milk of cows, buffaloes and other mammals. Research studies have shown that there are different variants of β -casein in milk evolved over hundreds of years due to mutation and selective breeding for high milk and protein yields. There are 15 known variants of β -casein out of which A1 and A2 are major. β-casein-A1 (alleged bad casein) differs from A2-casein only by one amino acid at position 67 (proline in A2 and histidine in A1). This substitution increased susceptibility of A1 β-casein to hydrolysis by digestive enzymes to produce physiologically active β-casomprohin (BCM), a decapetide.
The controversy is that one group of scientists claim BCM a cause of many health problems in human whereas other groups report beneficial effects of BCM and declare both types of milk safe for children and adults.
Is it true that Indian breeds of cows having humps are predominantly of A2 whereas European and American cows are of A1 type?
Genomic studies have shown that animals belonging to Genus Bos, which includes Indicus (Indian humped Zebu), Taurus (Exotic) and Yak were initially of A2A2 type only and due to mutation some animals became A1. But, with advent of selective breeding for high production, better fertility and protein quality, unconsciously A1 allele carrying bulls that were genetically superior were used in breeding programs. Artificial insemination (A. I.) of large number of cows with semen of such bulls multiplied A1 gene frequency over time. Several surveys have shown that A1 / A2 frequency is not breed-specific but area-specific. For example, in North America and North Europe A1 frequency in Holstein Friesen (HF) breed cow is very high (> 90%) but in German HF A2 frequency is high (97 %). In other countries A1 frequency in HF ranges between (40 – 65%). In Guernsey breed from USA / Europe A2 frequency in cows and breeding bulls is very high (> 98 %) almost equal to Indian breeds. In case of Jersey A2 gene frequency is higher (60-80%) globally. Kerry breed from Ireland and Spotted breed from Hungary has A2 frequency above 75%. In Indian hump breed cows A2 gene frequency is around 98 %. So it is preposterous to brand exotic cows as ‘dirty’ or ‘poisonous’. If we compare other milch species, buffalo, goat and sheep have only A2 genes hence milk from these animals would be exclusive A2A2 type.
Are Indian scientists silent on A1 / A2 research and situation is chaotic? This is mis-information propagated in social media to malign Indian scientists. National Bureau of Animal Genetic Resources (NBAGR), a renowned research institute in Karnal, has been active in surveying the A1/A2 situation in India since 2009. Their first report confirmed that A2 gene frequency in Indian breeds of cattle is around 98 % (almost 100 % in major milk breeds), whereas all the buffalo breeds studied were found to be of A2A2 type. Their further work in screening samples of HF, Jersey and crossbred bulls used in A. I. program also showed that these were predominantly carrying A2 allele. Recent studies published in 2012 also clarified that even in crossbred cow population predominant gene is A2. NBAGR has therefore rightly concluded that the situation in India demanded vigilance on breeding program but no immediate need to change breeding strategy. In April 2015 Indian Council of Agricultural Research, New Delhi has approved a study involving University of Punjab, NDRI and NBAGR to investigate and gather evidence about health safety of milk from Indian crossbred cows.
Is consumption of A1 milk cause of heart disease, diabetes and such other diseases in human? The scare about so called harmful effects of A1 milk in media is being spread by ill-informed group of activists. Firstly, one should understand that there is a huge difference between ‘causal factor’ and ‘risk factor’ as the later only increases risk of a disease but cannot cause the disease on its own. The published survey reports although point out risk association but overzealous campaigners have started labelling these as disease causal factors. The controversy started with papers published starting from late 1990s by Dr. Elliott’s group in Australia. One such paper has reported results of a survey wherein food consumption trends in 20 developed countries were compared with official mortality rates due to chronic heart diseases (CHD), juvenile insulin-dependent type I diabetes mellitus (DM-I) and other diseases. The survey reported strong association between high A1 β-casein consumption and CHD / DM-I. The association was found to be stronger in high altitude countries, such as North America and North Europe. India was not included as part of the study and moreover, it is not high altitude and has radically distinct socio-economic attributes. So these results cannot be extrapolated to India and the controversy for us stops there only.
Survey based epidemiology studies that compare situations in different countries in respect of food consumption and disease prevalence or mortality have several inherent limitations. These papers attracted lot of criticism as inferences drawn were overarching and erroneous. The assumption in the report was that every individual in the country was exposed to equal level of risk factor (for example A1-casein-milk), which we know cannot be true due to socio-economic differences within the country. Lastly results of such surveys provide flexible opportunity to the industry, media and scientists to pick up and magnify observations as per their perceptions. For example in these and other reports even rice, wheat and soy have been alleged to be comparatively stronger diabetogenic than milk but did not attract so much of media and public attention. Lastly, in such chaotic situation sane and independent voices of even eminent scientists group do not get attention. Dr. Truswell a renowned scientist from Australia in 2005 and European Food Safety Authority in 2009 after critically going through available literature published excellent papers rebutting claims about A1 casein milk but in media these are scarcely mentioned.
For establishing causal or risk association between factor and disease there are set criteria (also called Mills Canons); out of these two are considered critically important: (a) dose-response effect and (b) biological explanation with direct evidence. As per survey result although average A1- β-casein consumption in France and Australia was similar (0.3 g / day) the mortality rates due to CHD were reported to be 88 and 33 per lakh population, respectively. Sweden, Austria, Iceland, Canada, Germany have A1 β-casein consumption varying between 0.3 to 2.8 g per day the mortality rates due to CHD were 70-80 per lakh. Moreover, although A1 β-casein milk consumption patterns have not changed in USA, Australia, Switzerland over last decade but CHD mortality has dropped considerably. The hypothesis therefore fails to satisfy dose response as well as exposure elimination / reduction criteria.
What is the evidence of correlation to Type –I Diabetes mellitus?
Since diseases like DM-I is result of complex interactions between many factors the survey must be adjusted for known confounding factors else the association is likely to be distorted. In developed countries children consume cow milk proteins as ‘infant formula’, which is a very small proportion of national milk consumption and many formula have whey and reduced levels of casein. Scientists have earlier proved strong association between failure to breast-feeding during first three months of age and incidence of DM-I hence data should have been adjusted for this confounding factor. In many countries protein source in infant formula may originate from some other country where A1/A2 frequencies are different hence national averages of consumption may be misleading. For these shortcomings of such surveys epidemiologists are unanimous in view that comparison of data between the countries might at best be considered as the starting point for framing a hypothesis and conduct of experiments to gather direct evidence.
‘What about biological explanation revolving around BCM? To date most of the BCM effects reported in the literature are from the experiments done in petri-dish or test tubes. To exert biological effects on extra-intestinal organs, such as heart, brain or pancreas, BCM should be released in intestine after consumption of A1 milk, then it must be absorbed across intestine into blood and then taken to the target organ (for example pancreas in case of diabetes). There are no reports as yet to show that after consuming A1 milk in human BCM is released in intestine. Secondly, there is no proof that nascent BCM is absorbed intact across the intestine and enters in blood circulation. On the contrary there is unequivocal evidence that in healthy human maximum tripeptides can cross intestinal barrier intact. It is likely that 7- amino acid long BCM may be rapidly broken in intestine down to smaller peptides and absorbed. Larger peptides can cross intact only in leaky intestine seen in new-born infants for first few days and severe intestinal diseases. So the whole theory based on generation of BCM from A1 milk as cause of harmful effects has no scientific standing, as yet.
Are there reports to suggest beneficial effects of BCM? Yes, there are published papers in very reputed journals that BCM as well as other beta caseins have local beneficial effects. Scientists from France, Spain and other countries have provided evidence that BCM contributed to mucin production in intestine which has protective function hence could have dietary and health applications. Research papers published during 2012-2015 by Chinese scientists suggest that BCM might have protective role and prevent kidney complications in diabetes patients. In these papers too although BCM was fed to animals orally, but no evidence on its absorption was provided.
Are there direct experimental evidence in laboratory animals? A number of studies on DM-I in laboratory animal models have been published in reputed international journals. However, there is only one publication on association of CHD and BCM done in rabbit, which is not considered as a human model for this disease. BCM has been found to bind to specific opioid receptors and neural cells hence it is has been suspected to be one of the factors causing autism, schizophrenia and other neurological disorders. In these either cell culture was used or in laboratory animals BCM was injected intracranial, inside the brain or intra-peritoneal; obviously these are artifactual routes.
In order to obtain credible evidence of involvement of A1- β-casein milk and DM-I a multi-centre experiment in genetically susceptible mice model was carried out simultaneously at research labs in London, Ottawa and New Zealand. The diet to be fed to treatment group and various other control groups was prepared centrally and the researchers were kept blind to feed contents. The results from London and Ottawa laboratories showed that compared to mice fed on A1-β casein diet, incidence of DM-I was substantially higher in mice fed on control diet consisting of wheat gluten, soy and other ingredients. The New Zealand experiment conducted by a researcher who has been proponent of A1-harmful effects theory, was abandoned half way due to a disease outbreak in mice colony but for unknown reasons they did not repeat such a robustly designed experiment. Considering the available scientific data various panels of learned and reputed scientists have concluded that as yet there is no credible evidence to suggest that consuming A1 milk is related to CHD, DM-I, Schizophrenia autism, etc. There is also no evidence to suggest that consumption of A2 type milk would provide protection or sparing effects from these diseases.
What is the stand of Public authorities on this issue? Two international Study Groups comprising of renowned scientists, one in New Zealand and the other by European Union (European Food Safety Authority), have gone through available publications and evidences on the subject and have concluded that fear about A1 milk was unfounded. There are also independent panel reports which have concluded that as yet there is no clinching evidence to ring public warning. The controversy in few developed countries appears to be driven by commercial motives as in New Zealand a company called A2 Corporation has been formed which owns A2 related patents and brand name and has been demanding mandatory testing of animals for purpose of labelling. Obviously, a small group of ‘Activists’ type of researchers are driving this controversy but unless concrete evidence emerges India should not fall prey to this propaganda.
What are the lessons for India?

- In order to reiterate good qualities in indigenous cows there is no need to denounce exotic breeds or crossbreds.
- The hypothesis of A1 milk association with few chronic diseases drawn from a survey done in western countries’ population should not be extrapolated to India.
- Considering the contribution of buffalo, indigenous cows and crossbred population in India’s milk pool and based on the assumption that β-casein is 45% of total protein and that around 25% of the β-casein may be from A1 allele cows, the average consumption of A1 milk in India would be around 0.24 g / day; 5 – 10 times lower than countries surveyed. So there is no cause to panic.
- The Indian scientists should not consider the issue as buried but remain vigilant and monitor the situation periodically.
- The vested interest groups should not whip up passions and mis-information campaign but should leave such matters to the wisdom of our scientists and the scientists should become more vocal in stating facts.
- Lastly, if there is demand from consumers for A2 milk as a matter of choice, the Government of India and state governments should come up with policy guidelines and entrust the certification powers with the agency that is currently certifying organic milk, otherwise the consumers are likely to be rigged.
Download Reference at : a1-a2-references
Additional questions asked by the readers:
Whether Indian data proves that A1 milk is bad for health and hence we should focus more on our own breeds?
(Amrutdhara Gaushala, Karimnagar / Mayur Rathod, Raipur, Chattisgarh)
My critical review is based on analysis of published literature on the topic which also includes papers published by NBAGR and other groups in India. I don’t dispute the fact that Indian cows predominantly produce A2 milk. (note: buffaloes have fixed A2A2 genotype i.e.100% A2). The question I have addressed in the review is if there is enough credible evidence to indict A1 milk. As I understand from the published literature the answer is ‘No’, we need to wait for further evidence to emerge. Reference to second question I am a great but dispassionate proponent of Indian breeds of cows because of their good genetic characters such as heat tolerance, disease resistance and longevity. I am not too much worried about phenotypic characters but the aim should be to ensure conservation of good genetic characters and multiplying animals that are superior in performance. To some extent it is true that if our lot of cows if fed and managed properly, milk production can be increased by 15-20%, but the cost of feeding and revenue from milk output would not match. It is a different storey to rear cows on donations whereas rearing them from own investment is an economic activity for livelihood purpose. I have seen many Gir farms coming up with great national passion and praise to our cows but going out of business with same pace. The only long term answer is genetic improvement. On today’s cost unless a cow yields 2500 kg milk in a year its’ rearing would not be profitable to the farmer. Brazil in a span of 25 years have developed excellent purebred Indian cows (Gir and Kankrej) by employing scientific principles of breeding. India too can achieve this provided we allow scientific breeding by farmers which essentially includes selection of good animals and culling or disposal of inferior animals. Crossbreeding in Indian context assumes significant importance. Data indicates that increased milk production in India is not due to milk from Indian breeds but crossbred cows and buffaloes.
Isn’t the recent published report on side effects of A1 milk in human volunteers convincing?
(Ken Kii Koc)
The article published in European Journal of Clinical Nutrition on gastrointestinal problems associated with A1 milk is an interesting pilot experiment funded by the company which is marketing A2 milk and has exclusive IPR on detection kits. Obviously there is conflict of interest here. The design of experiment is not close to natural life situation; they fed 750 ml rice milk or 750 ml milk to adult volunteers daily for eight weeks. I don’t think this is normal milk consumption behavior of any Indian, American or European. Try out drinking 750 ml buffalo milk which is 100% A2 and you will have discomfort and soft stool. It is well known that cows that have high somatic cell count in milk also have high levels of anti-proteolytic factors (apha1 antitrypsin and others) in milk which could also cause similar symptoms. Realizing the shortcomings of their design the authors themselves are cautious to draw conclusion suggesting the discomfort could be due to intolerance to A1 milk (like lactose).
Which is dominant allele, A1 or A2?
(Dr. Santosh Singh Rathod)
In general cow population genotype for this gene would be A1A1, A1A2 and A2A2. A1A1 cows would produce only A1 milk and in the same way A2A2 genotype would produce only A2 milk. Since A1 and A2 are not dominant both alleles would be expressed if genotype is A1A2. That means milk will be a mixture of both A1 and A2 beta caseins. It is therefore necessary to consider genotype frequency rather than single allele frequency if cows are to be labelled A1 or A2 milk type.
Is it possible to identify A1 or A2 cow by phenotype characters?
(Dr. Santosh Singh Rathod)
No the only way to identify is genotyping employing RFLP-PCR test. The test can be ordered at National Dairy Research Institute for which you need to send blood or milk sample. For further instructions on sample collection and transport, requisition and cost interested readers may visit NDRI web site http://www.nbagr.res.in/offer.html
How to ascertain if the given milk is of A1 or A2 type?
(Dr. Santosh Singh Rathod)
There is no quick chemical test like fat or protein that can be done at the collection centre. The only method now available is PCR for which DNA from milk is extracted and A1 and A2 probe used to identify the genotype. This is in fact a big drawback because the trade otherwise will remain open to cheating common public as you would never be able to know unless an expensive test is ordered. How would the collection centre person identify if A2 milk has been adulterated with A1 ? In India therefore adapting this business model is not without major risk. Moreover there are no government agencies to certify A2 milk so you are solely dependent on honesty of the producers and marketers.
Is there a correlation between high milk production and presence of A1 allele?
No as yet. There is no such evidence available. It seems that in western world while intensively selecting bulls for high productivity this mutation gene which was low in frequency also got unintentionally selected and multiplied. Breeders started looking for its presence only after this controversy broke out.
Contributed by :
 Prof ( Dr ) Abdul Samad
Prof ( Dr ) Abdul Samad
MVSc, PhD ( Canada )
Dr Samad is a renowned herd health and veterinary medicine expert. Click Here for his short profile
The article is aimed at helping consumers understand the science behind controversies.
The content have been drawn from the published reports in peer reviewed and reputed journals. Pictures used in this page are from open source. Literature referred can be supplied on request.
You can write to Dr.Samad at drasamad11@gmail.com

